
Covid-19 and Coronavirus Lockdown. (Photo: husjur02/Shutterstock)
COVID Hysterics Hype ‘Positive Patients’ …and Cancel High School Football Game
‘Sacramento County’s COVID-19 hospital patient total jumps 48% in a week as uptick continues’
By Katy Grimes, September 11, 2023 2:45 am
“The number of hospital patients with COVID-19 in Sacramento County jumped nearly 50% in one week, reaching its highest level in five months, as the gradual increase in spread of the virus has yet to wane in California,” The Sacramento Bee breathlessly reported.
Oh holy @#$! We’re all going to die… (eventually).
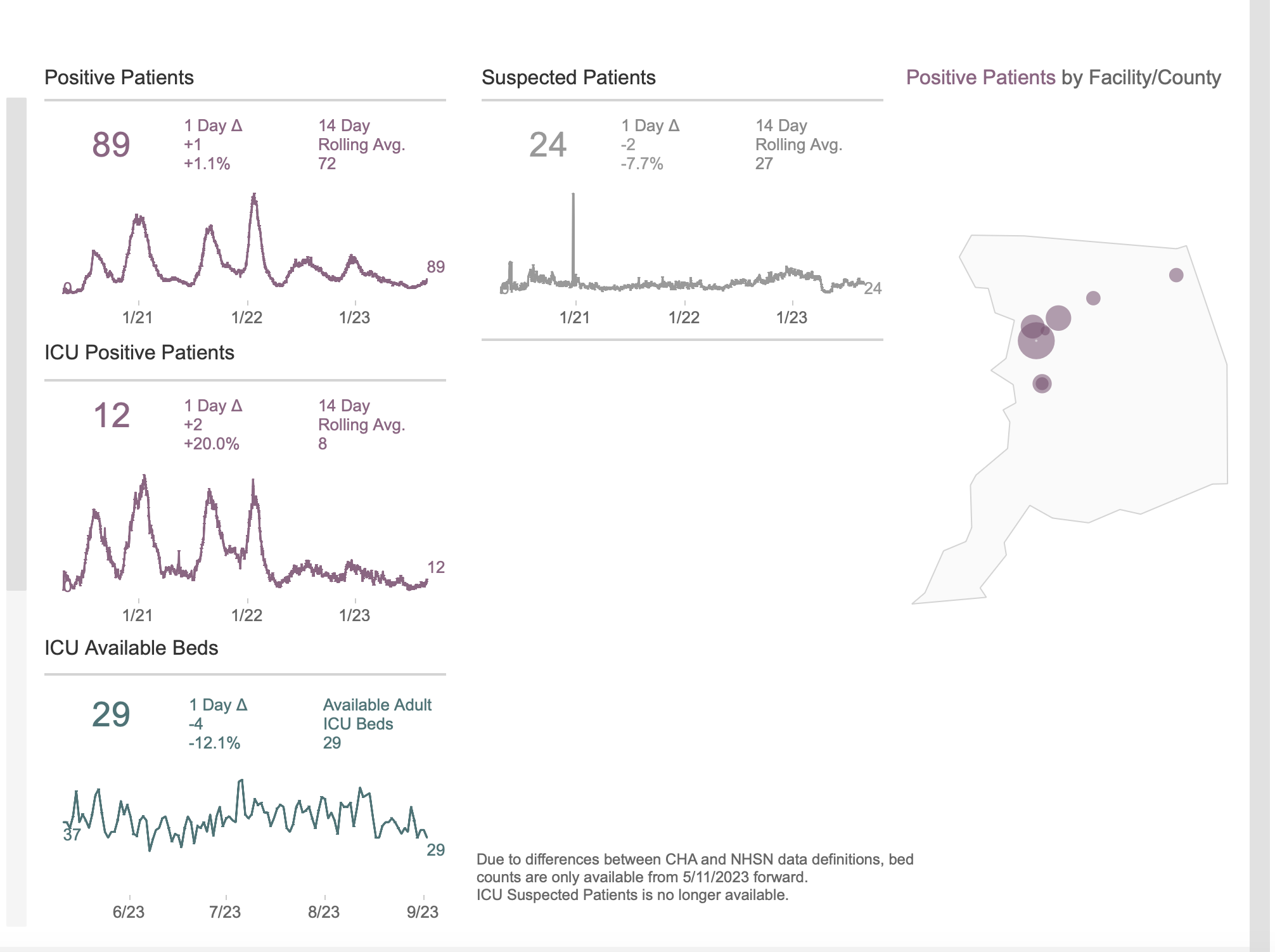
Wait. How many COVID patients are we talking about in Sacramento County? Am I reading this correctly – 89 total? Sacramento County has 1.5 million total population.
Last year at this time, there were 168 “positive patients” in Sacramento County, and 25 in the ICU, according to the California Department of Public Health. I don’t recall any headlines last year like this one from the Bee today:
Sacramento County’s COVID-19 hospital patient total jumps 48% in a week as uptick continues
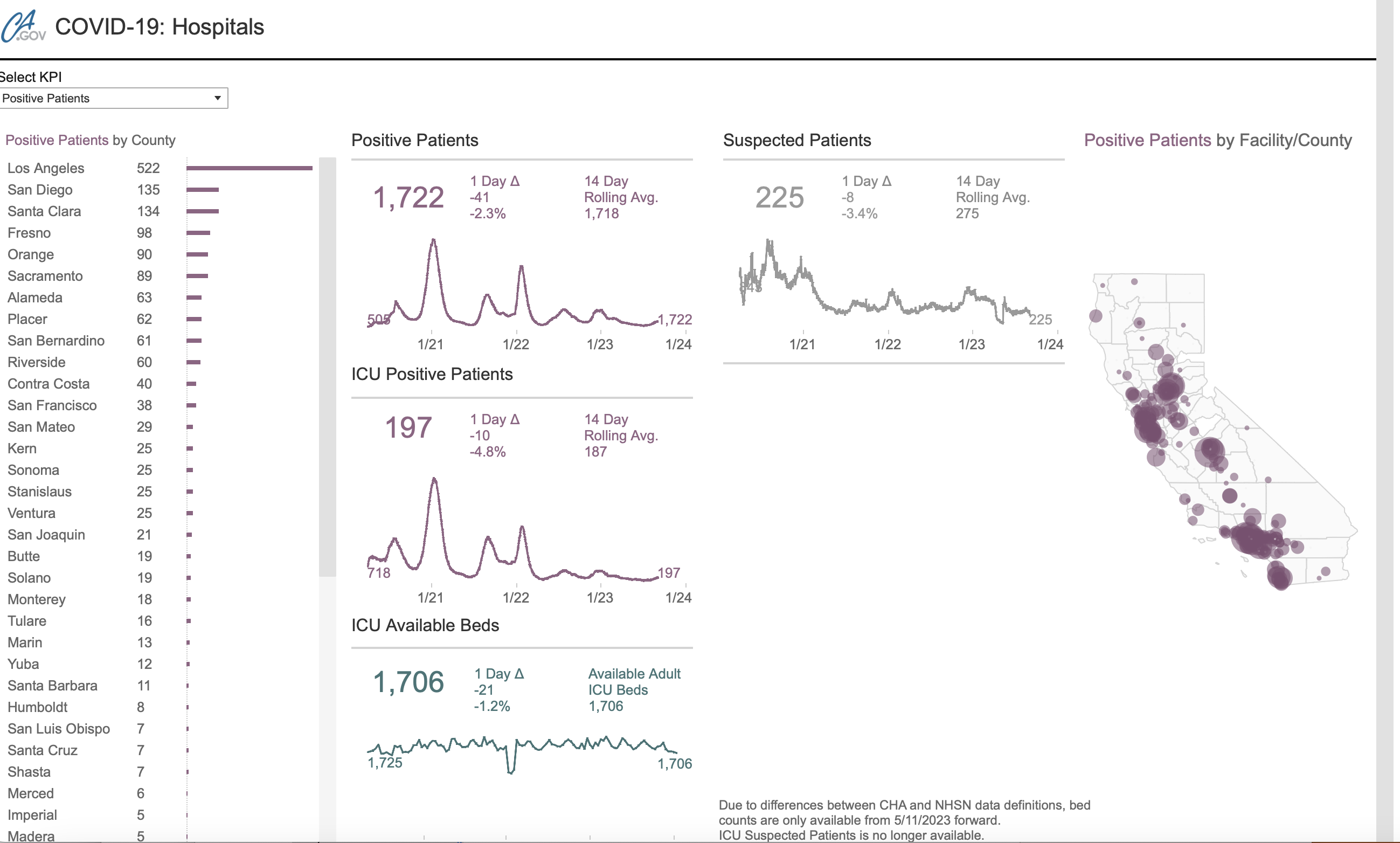
“There were 1,722 total hospital patients with COVID-19 in California as of Sept. 2, according to the most recent state data. That’s the same number of patients statewide as one week earlier, according to a weekly update Friday from the California Department of Public Health.”
1,722 total hospital patients with COVID out of 40 million people in California? Even with more people dying from Heart Disease and Cancer, it’s telling that public health officials are trying to increase fear in COVID again. The entire country can’t be locked down for heart disease or cancer, but they succeeded with COVID once already.
The CDC reports:
In 2022, approximately 3,273,705 deaths† occurred in the United States. The estimated 2022 age-adjusted death rate decreased by 5.3%, from 879.7 per 100,000 persons in 2021 to 832.8. COVID-19 was reported as the underlying cause or a contributing cause in an estimated 244,986 (7.5%) of those deaths (61.3 deaths per 100,000).
During 2022, the three leading causes of death were heart disease (699,659 deaths), cancer (607,790), and unintentional injury (218,064).

According to the CDC, “COVID-19 was the underlying cause for 5.7% of all deaths in 2022, decreasing from 12.0% (416,893 deaths) in 2021. Heart disease and cancer deaths increased in 2022 compared with 2021 (accounting for 695,547 and 605,213, deaths respectively), while deaths associated with COVID-19 decreased.”
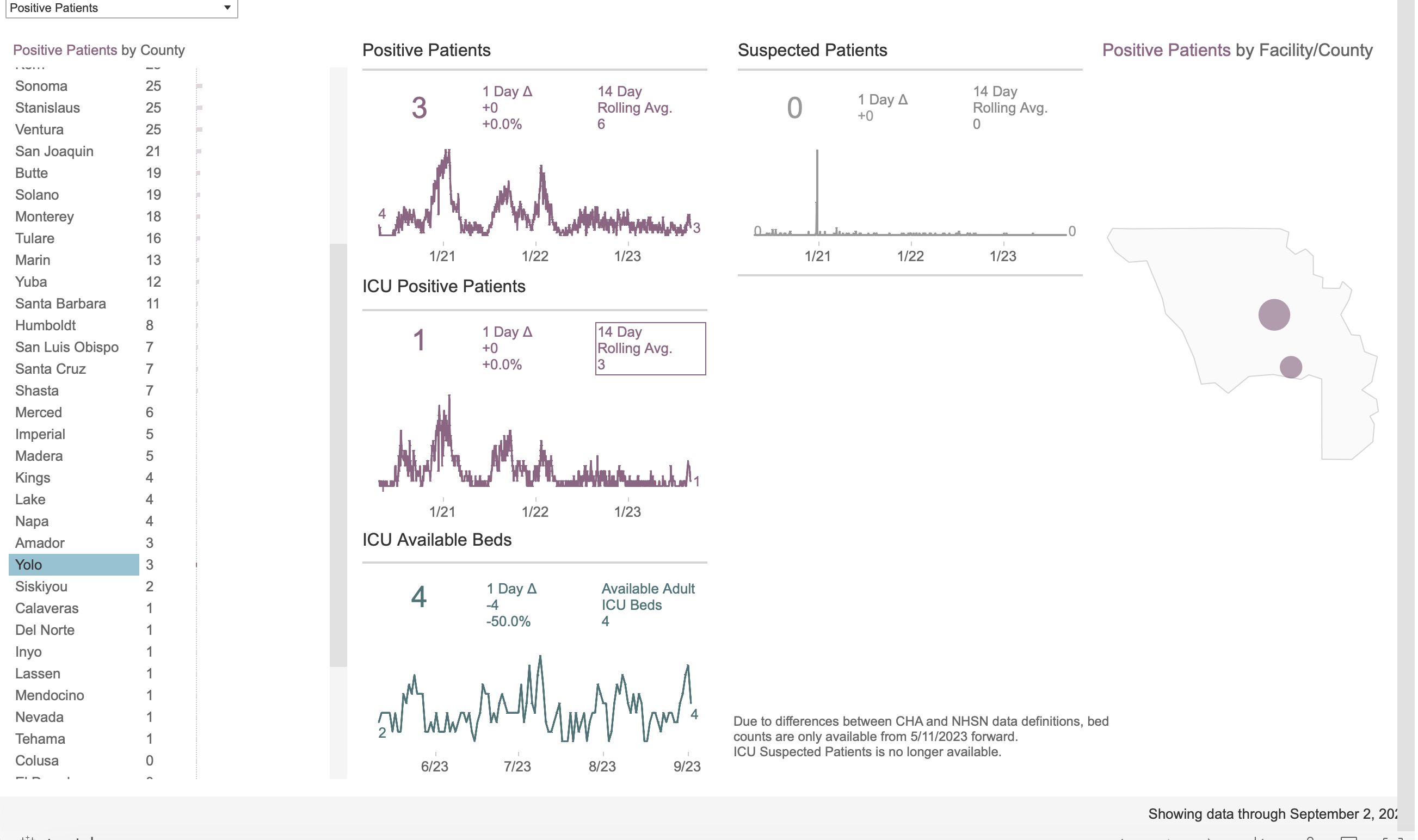
Locally, Esparto High School in Yolo County cancelled a football game Friday night because 6 players tested positive for COVID-19 — and 7 players were out with injuries. I assume the players are required to test for COVID? The school district said the game cancellation was necessary because the players could pass COVID to the other team.
I’m willing to bet the players weren’t sick – they just tested positive.
Here are all of Yolo County’s COVID stats: 3 COVID positive patients and 1 in the ICU – out of 222,000 total population.
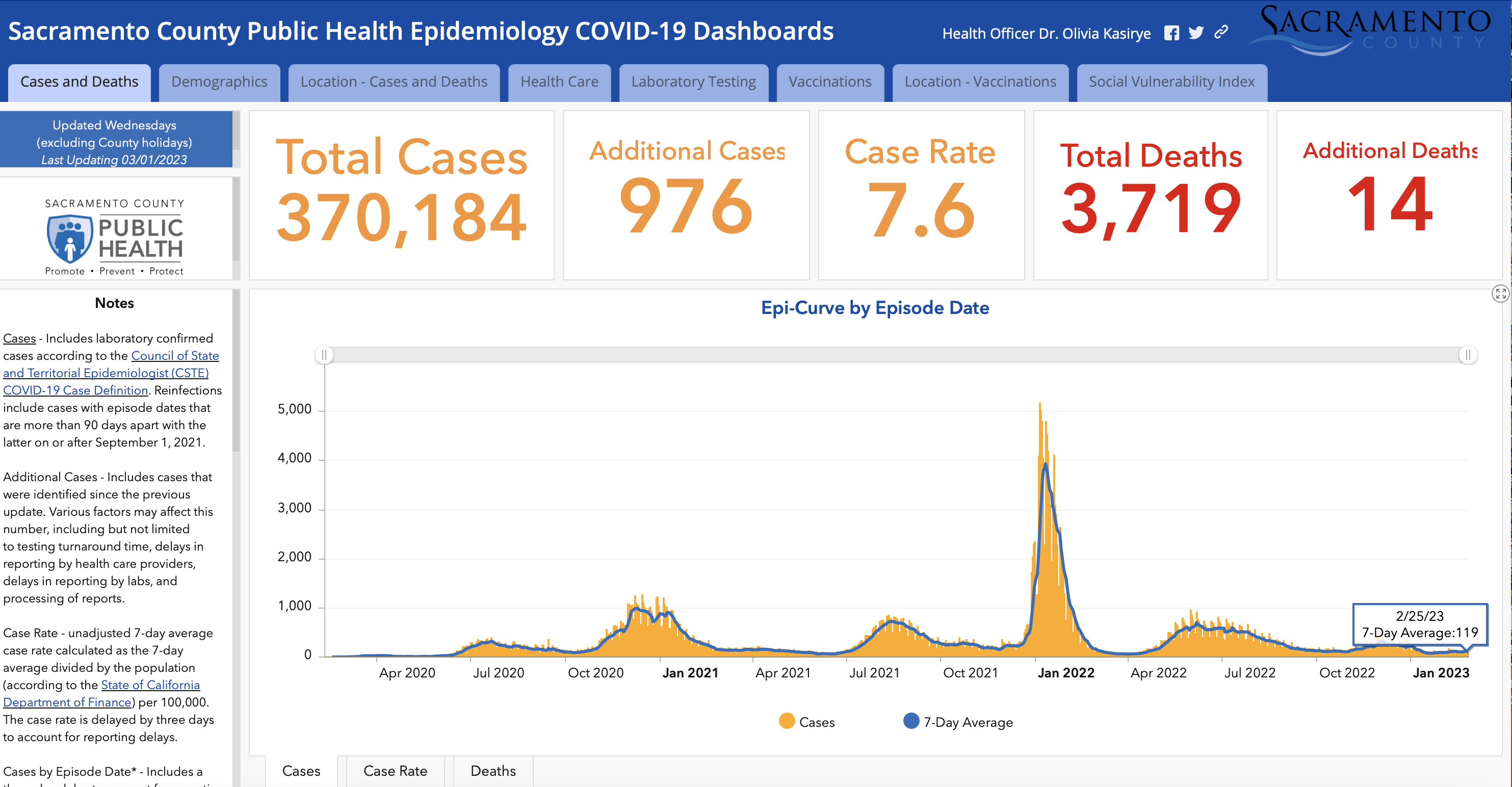
Oh – Sacramento County still hasn’t updated its COVID dashboard since February 2023 – they must really be concerned about it:

A California native and Navy mom, Katy lives in Sacramento, CA.
- Energy Company Warns CARB on ‘The Stark Reality’ Driving In-State Refining Capacity to Zero of CA’s Remaining 7 Refineries - February 28, 2026
- CAL DOGE Investigation: $1 BILLION California Solar Program Instead Funded Democrat Voter Registration & Activism Efforts - February 27, 2026
- Could President Trump End the Income Tax? - February 26, 2026



Just a reminder that all low prevalence screening tests have no clinical diagnosis validity. If the prevalence in the general population in percentage terms is below the error rate for the test then most positives are false positives. This is very basic math.
Although the COVID test makers claim a sensitivity/specificity rates of up to 90% those are only in very controlled lab conditions. Or by finessing the numbers. In real world screening its more like <70% sensitivity and <80% specificity. Maybe. Plus the false negative rate even in a controlled environment is over 50% for active infections. These tests just dont catch infections during most of the active infection phase.
So if a COVID test result is positive its a low probability you have a active SARs Cov2 infection. Statistically speaking. Unless you have specific symptoms or show signs of early stage pneumonia. Then you might have it. Or one of the other 20 common viral respiratory infections. Like the 4 other corona-viruses. Which all have the same symptoms. And all have much higher prevalence rates at any given time in the general population.
Remember. Most doctors not only cannot write legibly but also cant do math. And must have slept through the epidemiology classes in med school as well. As the last fours years have proved.
And the majority of public health officials in California have absolutely no relevant medical qualification. None. And those that do the qualification were acquired many decades ago and none of them has any relevant clinical expertise. In other words, charlatans.
Tfourier, thanks for the head’s up regarding the lack of validity in Covid testing. Unfortunately, those who reaped financial and political rewards from the worldwide Covid scam have no incentive to let up. I still see plenty of gullible people walking alone or driving alone while wearing masks. Billions of dollars will be made when corrupt government agencies mandate the next round of useless and potentially harmful non-vaccine vaccines.
Tfourier, I don’t know where you came up with less than 80 percent specificity. A JAMA study (https://jamanetwork.com/journals/jama/fullarticle/2788067) reviewed antigen tests in 2021 and found a 42 percent false positive rate, using PCR as a ground truth standard. Presumably the tests have improved in the intervening 2 years, but let’s accept that. The question we should ask is “if 6 members of a high school team test positive, what is the likelihood that none of them actually are infectious with Covid?” Can we stipulate that “positive PCR test” is a good stand-in for “infectious with Covid?” Can we also stipulate that the team has 40 members? I don’t know the exact number, but do you agree it’s reasonable? One more stipulation, that false positives among players are uncorrelated. That matters because, per the JAMA article, false positives are correlated by test lot number and we don’t know if all the tests came from the same lot. With these stipulations, we can calculate the likelihood that none of the team have Covid. It’s 40-choose-6 (the binomial probability function) times 42 percent false positive rate to the 6th power times 58 percent true-positive rate to the 34th power (34 being the number of players who tested negative). That’s 0.09, or about 9 percent. So the likelihood that the team DOES have a Covid-infectious member at the time of the test is 91 percent. Considering Covid incubation time, that’s a minimum because other infected members haven’t reached the positive-result antigen threshold.
Given 91 percent probability that at least one player has active infection from a highly contagious virus, Esparto HS made the right call. The “hysterical” actor here is Katy Grimes, who obviously didn’t check the math either. I accept that, since I’m really good at math and most people aren’t, we can forgive Katy her error. But then we should also ask Katy to just report the facts, and not her misinterpolations from them. At least those doctors who “cant do math” know that they aren’t doing math, and just follow what experts tell them.
Public Health officials are much more competent, especially as a group, than you give them credit for. Many of the people who do the math have degrees in something other than medicine (like I do). The people who do the math cooperate with the people who have the medical degrees and the people who have many other skills the have to come together to make Public Health happen.
Lets deal with some of your points.
1) SARs CoV 2 RT/PCR reagent specificity. The calibration used for the RT/PCR initial reagents was unique markers for SARs CoV 2 genome v the four other general circulation HCOVs. 229E, OC43 etc, Problem is the number of unique refence database markers for the other HCOV’s is very small and HCOV’s are very mutagenic and there is almost no common (or uncommon) variants in the genomic databases. Compare and contrast with influenza. Basically little or no research was done on HCOV’s prior to 2020 so there is almost no hard data. Compare with influenzas. rhinoviruses, RSV etc
So the math used to calculate the RT/PCR reference reagent specificity was wrong. Very wrong. The necessary resolution is just not there. By almost an order of magnitude by the look of it. Then the FDA decided that all future reagent approval was to be against one initial benchmark reagent not the standard calibration tests used in the past. .
If you dont see the huge problem with that then you really don’t understand even the basic math involved.
And thats only the start of the problem. Do you know why Kary Mullis said never ever use PCR for diagnosis ? Because he knew the limitations and he knew the math.
In fact for SARs CoV 2 the FDA threw out all previous rules. Everything since the 1960’s. Ignored. Like approval to manufacture is not the same as a 505(b)(1) approval. Not even close. Very deliberate obfuscation.
Have you checked any of the reliable papers on actual accuracy of clinical lab tests. When done for the general public in high volume not in a low volume lab calibration test for the FDA. Thats where I got my real world numbers from. So pretty eye watering numbers in those high volume test accuracy reports.
2) From the math you quoted it’s obvious that you dont understand the math. You really dont. This is very basic sampling theory in statistics. The Type I and Type II errors in low prevalence screening tests.
Do you know why before March 2020 the protocol for using RT/PCR in serious respiratory infections was only after at least two other sign of pneumonia had all ready presented themselves (x ray and bloods) . Because by that stage the prevalence probability was now way above the typical testing error rate. So the Type I / II error rates were now in the range of an acceptable clinical tests. 80% true positive / 5% false negative.
There is no scenario in how RT/PCR has been used since March 2020 where it is a valid clinical test. By pre March 2020 protocols. Because of the math.
3) With the lateral flow test where do you begin. Its just like RT/PCR except the math is a lot lot worse. The numbers in the FDA filings for these tests are a total train wreck.
I am a math guy with a hard science background. So when I read the papers, reference books and the public health orgs datasets the first thing I look at – is the math correct. Or even close to correct. In 90%+ of bioscience / medical papers I have read the conclusions in no way reflects or often even matches the math. Usually riddled with very basic math errors.
You know the old joke about the hard science people v soft science people… It totally true.
4) I looked at the resumes of the all the big city public health officials in CA back in 2020. I stand by my statement. Only one third of them had any kind of medical qualifications. And those that did had zero or near zero relevant clinical experience. All career professional public health bureaucrats of one form or other. A PhD in “public health” is little better than one in sociology.
5) SAR CoV 2 is now the fifth general circulation HCOV. It has the same kind of pathology of the other four. It has the same kind of IFR and CFR (and R0) as the other four once you factor out the massive misclassification of WITH/FROM deaths since March 2020. By changing the clinical criteria. Compare the numbers from say Norway were the datasets is pretty clean with NY or CA were the datasets are pretty much worthless. Just like those from Italy and Spain and a whole bunch of other countries. China anyone?
SAR CoV2 like SARs CoV 1 mostly causes death by pneumonia / ARDS and seems to be mostly a HAI. A hospital / heath care related infection. Just like pneumonia. Who spends the most time in hospitals etc . Old people. Counties with low HAI rates had low mortality rates from SARs CoV 2. Those that had high HAI rates..
For the vast majority of people who have a low PSI/PORT score the health risk from SARS CoV 2 is no different from any other HCOV. Although the initial infection as its novel can be a bitch. That loss of smell / taste through ORN infection and incredibly sore nose I had at the end of Feb/ start of March 2020 was no fun at all. The one specific symptom for SARs CoV 2 infection. Got it directly from the same place the initial US infection came from. Northern Italy.
It was still just a bad cold compered with Swine Flu in 2009. H1N1. Now that was really nasty and took me months to recover from. I was not old enough to be exposed to epidemic H2N2 in 1957 so did not have any cross immunity. Because thats how H1N1 eventually played out. Old people had a unexpected low mortality rate in 2009/10 due to prior cross immunity to H1N1. The same cohort who died in 2020.
The number of people who will die due to disrupted heath care (and other causes) because of the hysterical public health response in 2020 will vastly outnumber the relatively small number of extra people who died of pneumonia in Q2/Q3 2020. Mostly substitute cause deaths I might add by the look of it. Thats why mortality never went outside the 10 year range. Except for one age group in Q2/Q3 2020. Is that even a pandemic? By the traditionally accepted criteria.
The people who died almost all had low YLL scores but most of the people hurt by the hysteria are mostly high YLL score. So by any traditional public health measurement the response since 2020 has been the biggest public health catastrophe in the modern era. Not the emergence of a novel strain of HCOV but the public health response to it.
This will set back public health decades by the time it is over. Due to the current generation of public health officials criminal incompetence.
Tfourier: When you pose a challenge like “Have you checked any of the reliable papers on actual accuracy of clinical lab tests,” it’s hard to know how to respond. Apparently you have somewhat non-mainstream opinions of what is “reliable,” so without any specific reference I don’t know what you mean. I’m pretty sure that the typical CaliforniaGlobe reader is completely lost, and simply believes you because they don’t like the conclusions I reach though my scientific consensus-based approach.
Also, you’re arguing about process failures, but policy has to be based on facts, not whether the process is perfect or whether you think PH officials are competent. The actual results are 6 positive tests among the players for a disease that killed over a million Americans. You can’t just dismiss this without some idea of how risky it is to ignore 6 positive results. Suppose we were to take your (perhaps supportable) word for it, that even the PCR test is only 80 percent specific. At worst, it has a 20 percent false-positive rate. Applying that factor to the JAMA result (antibody has a 42 percent false-positive rate relative to PCR), we could have as much as 50 percent false-positive rate for the antibody test, relative to actual Covid infection. That still suggests on the order of 3 true positives and over 85 percent chance of at least 1 true positive among the 6 players. Is the school really supposed to let the kids play despite an 85 percent chance they will be in contact with at minimum one infectious player?
As for comments by Kary Mullis (who died before Covid emerged, BTW): So what? Felix Bloch got a Nobel prize for NMR, and he told me personally (and not just me, lots of people) that MRI would never make useful medical images because it would not have enough signal-to-noise. I took a job in the MRI industry anyway and we made great images that proved him spectacularly wrong. The opinions of dead Nobel laureates about what can or cannot work aren’t worth as much as people might think.
Thank you for the expertise you provided, tfourier, and for your time.
Always appreciate your intelligent posts.
Now let’s examine the number one cause of death in the year 2022, HEART DISEASE.
What were the numbers before the mRNA shot roll out?
Will we continue to see the deaths from heart disease increase?
Will we continue to see young athletes in the prime of their life drop to the ground during a cardiac arrest event?
Will we continue to see once healthy friends and family newly diagnosed with heart issues and aggressive cancers?
Instead health officials decide to close down a Friday night high school football game due to a slight increase in covid “cases”.
Never let a crisis go to waste, especially when it comes to the celebration of a high school sport tradition.
Be afraid people, very afraid!
It is not a weakened , engineered virus that we should be fearing.
As I wrote in my reply to Tfourier, Esparto HS made the right call. There was a very high likelihood that at least one player had Covid and is contagious. Covid killed a lot of Americans; let’s not let disease complacency kill even more of us.
Of course death follows each of us, every single day. That is part of the human condition that will not change. Ever. Rather than fearing misplaced suspicions of authority figures, you’d be better served if you learn to “fear” your own risk factors, such as body weight, glucose levels, environmental toxins, poor diet or inadequate exercise. Don’t let misplaced fears distract you from your own opportunities to extend your life and to enhance your enjoyment of it!
Gee, thanks for the advice, S.F. aka Concerned Citizen.
As I have stated before I do not fear this or any virus and lead a very healthy lifestyle.
Interesting you would think the high school administration made the the right decision.
Katy put up the graphs. By the way how many young healthy people under the age of 18 have of died from this engineered virus?
[“Many American’s died. Let’s not let disease complacency kill even more of us”]
Good stuff there @SF, keep pushing the fear! I better go get a 4th booster and mask up and do what the Public Health Officials mandate!
I actually find your advice and reasoning very contradictory.
I also much appreciate @Tfourier’s response to your criticism. It coincides with what I have read as well.
Have an enjoyable day @S.F. aka Concerned Citizen.
May God Bless you.
Death, Taxes, and election year viruses
all certainties even more now with rigging a steal