
Sacramento homeless camp. (Photo: Katy Grimes for California Globe)
Spending on CA Homeless Increased Street Population, with Scant Treatment for Mentally Ill
California earns a D- grade on the lack of psychiatric care
By Katy Grimes, June 4, 2021 2:32 am
Earlier in the year, California lawmakers proposed a $20 billion plan to give California cities funds to combat the homeless epidemic. Gov. Gavin Newsom proposed $12 billion in spending, which seems only to entice more homeless people to move to California, and grow the mentally ill drug addicted street population.
In a May statement, the Governor’s press office said:
Governor Newsom’s $12 billion plan to tackle the issue of homelessness will be the largest investment of its kind in California history. This investment will provide 65,000 people with housing placements, more than 300,000 people with housing stability and create 46,000 new housing units.
In 2019, California had roughly 134,000 homeless people, amounting to one-quarter of the nation’s total homeless population. Some in the state admit to 161,000 homeless now, but looking at the governor’s numbers, it’s clearly much larger.
In April, Gavin Newsom bragged that California set up a national model to “solve homelessness” by converting hotels into homeless housing. “Project Roomkey” hasn’t exactly been a success, with likely 200,000+ homeless in the state. And reports of scores of unused trailers in several cities isn’t helping.
Untreated homelessness is so bad in Los Angeles, a U.S. District Court Judge ordered the city and country of Los Angeles to offer housing or shelter to the entire homeless population in the Skid Row neighborhood by October.
And that is the real problem – the “homeless” are mentally ill, drug addicted street people who aren’t getting treatment. Many aren’t as much “unhoused” as they are “unsober” and “unhealthy” mentally. A friend in law enforcement said that for most of the drug addicted, mentally ill homeless, they can’t make it in society and never will. They need more than a trailer or old hotel room – involuntary psychiatric care is what mental health experts say is needed.

California’s State Auditor Elaine Howle issued a rather scathing audit in February over the management or mismanagement of Homelessness in California. She said that the state continues to have the largest homeless population in the nation “likely in part because its approach to addressing homelessness has been disjointed.”
Howle said “At least nine state agencies administer and oversee 41 different programs that provide funding to mitigate homelessness, yet no single entity oversees the State’s efforts or is responsible for developing a statewide strategic plan.”
The state’s plan to mitigate homelessness is not designed to achieve this, as the audit shows. Because if the 9 agencies and 41 different programs did mitigate homelessness, they would no longer be needed, the federal and state funding would dry up, and public employee union jobs would be lost. In California, no program ever sunsets.
California has spent $13 billion in just the last three years on the massive homelessness problem. The auditor said the approach to dealing with homelessness is so fragmented and incomplete it actually hinders efforts at getting people into stable housing. And the auditor found the Continuum of Care organizations (CoCs) “do not consistently employ best practices to improve homeless services in their areas. The five CoCs we reviewed do not adequately conduct a comprehensive annual gaps analysis,” the Auditor reported. And two of the CoCs don’t even have current comprehensive plans.”
“Last year, Newsom vetoed a bill that would have created a uniform data-collection system on homelessness spending, saying the measure was duplicative and would create additional and unnecessary data collection costs,” KCRA Channel 3 reported. “However, the auditor found a lack of coordination between agencies, and largely, no accountability by any agency our the task force.”

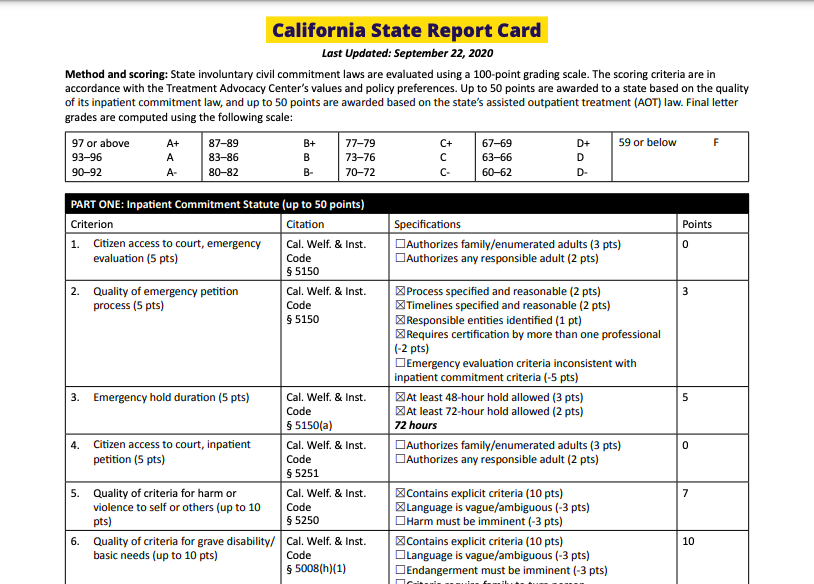
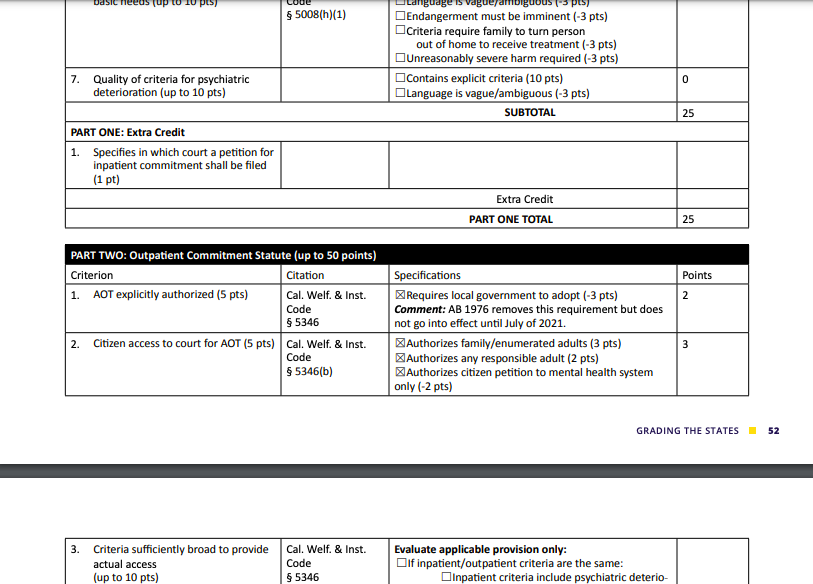
The Treatment Advocacy Center, whose goal is “Eliminating Barriers to the Treatment of Mental Illness,” issued a recent report on the lack of psychiatric care available in the 50 states. California earned a D- grade.
“Grading the States: An Analysis of U.S. Psychiatric Treatment Laws examines the laws that provide for involuntary treatment for psychiatric illness in each state. For each state, we analyzed whether an individual who needs involuntary evaluation or treatment can receive it in a timely fashion, for sufficient duration, and in a manner that enables and promotes long-term wellbeing.
To do so, we asked a crucial question: Does the state law allow an individual in need of involuntary evaluation or treatment to receive timely care, for sufficient duration, in a manner that enables and promotes long-term stabilization?”
The report explains: “Public mental health is primarily the responsibility of state and local government. State legislatures pass laws establishing the criteria and procedures for when and in what manner the state may override an individual’s refusal of mental health treatment.”
Each state was evaluated on the following criteria and recommendations based on the Treatment Advocacy Center’s analysis of the treatment laws in each state, and key components of an ideally functioning system of mental illness treatment laws.
These are the Treatment Advocacy Center’s Policy Recommendations
- The time limit for an emergency hold should not be less than 72 hours with 48 hours as an absolute minimum.
- Emergency evaluation laws should provide clear guidance for practitioners, law enforcement and families. Any responsible adult or, at a minimum, a guardian or family member, should be authorized to petition the court for both emergency evaluation and inpatient civil commitment.
- Criteria for danger to self should expressly include grave disability and psychiatric deterioration.
- Criteria for grave disability should not require either unreasonably severe harm or for families to be required to deny assistance.
- Criteria for psychiatric deterioration should allow consideration of treatment history and the likelihood of future psychiatric deterioration without treatment.
- Criteria for danger to self or danger to others should not require imminent harm.
- Assisted Outpatient Treatment (AOT) criteria should allow consideration of at least three years of treatment history and must be suitable for outpatient use.
- AOT criteria should not place unreasonable limitations on eligibility.
- Any responsible adult or, at a minimum, guardians and family members should be authorized to petition the court for AOT.
- AOT procedures should be described in sufficient detail to provide guidance to practitioners and to make maximum use of the “black robe effect.”
- The duration for an initial AOT order should be a minimum of 90 days, and renewed orders should be for a minimum of 180 days.
The raw scores were then converted into one overall letter grade based on total points earned on a 100-point scale. Conversion of raw scores to overall grades 97 or above:

They explain about the quality of involuntary treatment laws and summarized the results of their analysis of state practice for civil commitment laws and our grades for each. “A detailed breakdown of the scoring for each state, as well as specific findings about the strengths and deficiencies of each state’s laws, may be found within the individual state grade sheets of this report contained in Appendix A. Of the fifty-one jurisdictions (fifty states plus the District of Columbia), ten earned an A (a score of 90 to 100) while eight received failing grades (a score of 0 to 59). Minnesota achieved the highest combined score, with 97 out of 100 points. Maryland received the lowest combined score, with 18 out of 100.”
The Treatment Advocacy Center also compared states to the other states in each category: Emergency (out of 15), Inpatient (out of 35), Assisted Outpatient Treatment (AOT) (out of 50).
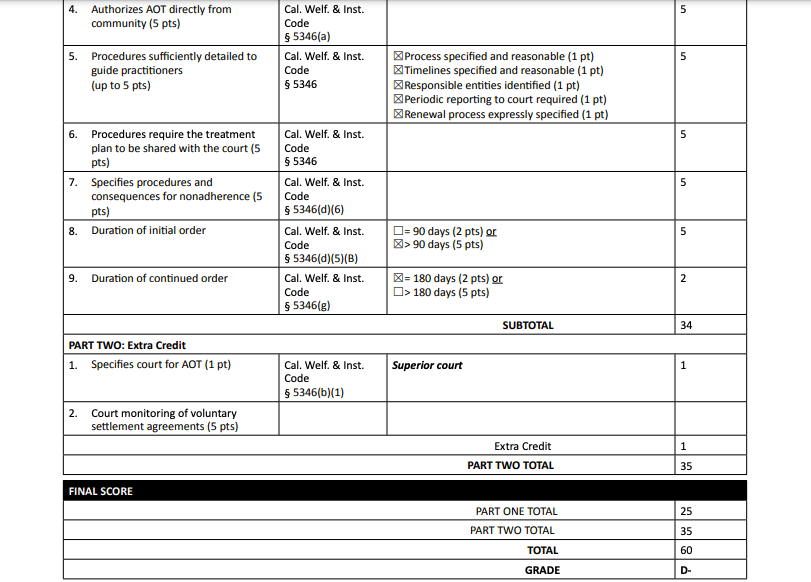
California earned a score of 8 in Emergency (out of 15); 17 on Inpatient (out of 35); and 34 on Assisted Outpatient Treatment (out of 50).
In the Statutory Barriers to Treatment, the Treatment Advocacy Center recommends against requiring certification by more than one professional in order to initiate emergency evaluation. “We found that five states – Alabama, Alaska, California, Idaho, and New Jersey – have adopted laws with this onerous requirement, which poses an artificial barrier to treatment.”
California did not fail in every category, but the D- grade indicates there is a lot of room for improvement in the psychiatric care available for California’s mentally ill living on the streets – or lack thereof.
As the California State Auditor reported, her office reviewed a number of other states which have charged a single agency with addressing homelessness statewide and tracking funding information centrally. “These other states have fared better than California in stemming the number of people who experience homelessness.”
Below is California’s report card from the Treatment Advocacy Center. You can read their report here.

A California native and Navy mom, Katy lives in Sacramento, CA.
- While Newsom Fiddles, California’s Gas & Oil Crisis Ramps Up with Tensions Between the US and Iran - February 22, 2026
- Trump Responds, Issues Global 10% Tariff on all Countries - February 21, 2026
- What is Trump’s Plan B After Supreme Court Strikes Down Tariffs? - February 20, 2026
RELATED ARTICLES
-

-
 January 16, 2020
January 16, 2020 -
 December 21, 2019
December 21, 2019
Because pouring more money down the Social Services rathole always works, in the end.
We need to change the language of the “homeless” issue debate. Stop calling mentally ill, violent drug addicts “homeless” . Only a small percentage of people living on the street are truly homeless and those tend to be without housing for short periods of time due to things like the covid shutdown taking away their jobs. Call it what it is – the mental illness pandemic fueled by out of control drugs and government money.
Katy, you have been an invaluable asset to those of us that are locally affected by the inadequate response from the state. Local municipalities are having great difficulty dealing with this issue.
Again, it is a dereliction of duty to ignore the Auditor’s report. The root cause is being ignored and it is very frustrating to watch. The majority of young homeless are left on the streets to rot in their hell , this state enables them instead of truly getting them the shelter and rehabilitation they need!
Thank you Cali Girl. This one issue could be the tipping point for California if not honestly addressed.
I commend Katy for an excellent well documented topic. Here in Bakersfield California, our city is dumping forty five million into building an 85 bed housing project. To my estimate, what has actually been created is another Industry to wealth building designed primarily too enrich government (workforce) including Private sector Construction companies whom freely over estimate cost to build as they wish.
As to shrinks availability to even began a treatment plan, mandates evaluations, concept of treatment options, more hours in documentation amounting to a small army of administrative/support staff working full time. Mental illness is not easily treatable. It can take years if not longer.
Then, exactly how many mental illness professionals are there? This second try making a private appointment? Eight to Ten weeks out. Hmmm.
I believe in or [about] 1982 the courts ruled against states mental health institutions being closed down for involuntary commitments. This lead to thousands of wards being released too the streets of every town and city immediately becoming a whole new challenge to law enforcement and local county mental treatment facilities. One or more judges unknowingly caused this vicious human debauchery we all see today.
Comrades
Time for targeted intervention….save the best, hospitalize the infirmed, aggressively deal will drugs at all levels….use appropriate sections of prisons for assistance…..
Lots of manual labor needed in the forests. Tent camps worked just fine for Roosevelt’s programs.
We have, supposedly, a California Conservation Corps now. We haven’t made the use of it that we should have.
Sorry, but the pols do not care about the “grade” they get about this issue. They care about the distribution of taxpayer money they can get to their supporters. The camouflage for this shakedown is compassion, but compassion for the needy or for the community does not have anything to do with it. Why do they act with such impunity? Because certain precinct captains are bought and paid for!
Katy……please follow the money and expose these phonies for what they are!!
Hopeforsacramento.org
Pouring good money after bad is ridiculous! It is obvious that this isn’t working for anyone, least of all the “homeless”. Mental hospitals should be re-opened for all the mentally ill people on the street and elsewhere, and it should be involuntary. That would be a much better use of our tax dollars. Some of these people will never get better; others will be able to get back into society. Creating more and more agencies, with all the costs involved, just wastes more tax dollars. And as the article says, once those agencies are formed, they never go away. Why should the taxpayer bear this burden?? The answer is: WE SHOULDN’T!!
But, but, but….
Labeling people as mentally ill is MEAN…. and possibly RAAAAACIST….
I saw it on CNN!!!
We are led by absolute IDIOTS!!!